






Femoral hernia
A femoral hernia is a groin hernia.
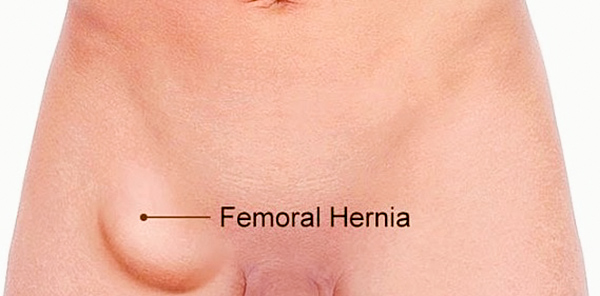
It often presents as a small swelling just below the groin crease, and is often mistakenly thought of as a swelling on the inside of the top of the thigh.
It often presents as a small swelling just below the groin crease, and is often mistakenly thought of as a swelling on the inside of the top of the thigh.
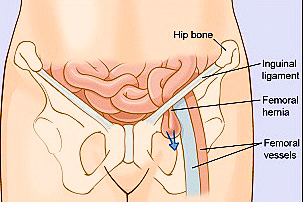
It occurs through the femoral canal – a natural occurring canal located between the femoral vein and the pubic bone.
Femoral hernia.
Symptoms and signs
Small to moderate hernias
These hernias are quite often asymptomatic—with no pain or bulge. Because of this, femoral hernias are ‘dangerous’, as they only become noticeable with strangulation.
Large hernias
These may present as a bulge in the groin near the upper thigh. There will be discomfort or pain in the groin area. It is also possible to feel some pain in the hip area too.
Strangulated hernia
The patient presents with:
These hernias are quite often asymptomatic—with no pain or bulge. Because of this, femoral hernias are ‘dangerous’, as they only become noticeable with strangulation.
Large hernias
These may present as a bulge in the groin near the upper thigh. There will be discomfort or pain in the groin area. It is also possible to feel some pain in the hip area too.
Strangulated hernia
The patient presents with:
- severe groin pain that occurs suddenly
- nausea, vomiting
- abdominal bloating/distention.
Risk factors for femoral hernia
Female
70 % of femoral hernia occurs in female. This is probably due to the larger female pelvis, hence a larger femoral canal.
Middle age
Chronic straining of the abdominal muscles causing a weakening of the muscular wall. Factors that can precipitate chronic abdominal wall straining include:
70 % of femoral hernia occurs in female. This is probably due to the larger female pelvis, hence a larger femoral canal.
Middle age
Chronic straining of the abdominal muscles causing a weakening of the muscular wall. Factors that can precipitate chronic abdominal wall straining include:
- obesity
- pregnancy
- repeated heavy lifting
- chronic coughing.
Repair of femoral hernias
Femoral hernias may be repaired through an open (traditional) repair or by laparoscopic (keyhole) repair.
Open femoral hernia repair
The incision is at the groin crease. The hernia is identified and reduced. A small mesh plug is placed into the defect and sutured in place. The skin is then closed with absorbable suture.
Laparoscopic repair
Three small cuts are made in the skin above the groin.
The space behind the muscular layer (called the extraperitoneal space) is enlarged with special surgical balloons. A telescopic camera is used to visualise and locate the hernia. This is then ‘reduced’ (returned to its normal place).
A mesh is then placed to cover the hernia defect. The skin incisions are then closed with absorbable sutures.
The space behind the muscular layer (called the extraperitoneal space) is enlarged with special surgical balloons. A telescopic camera is used to visualise and locate the hernia. This is then ‘reduced’ (returned to its normal place).
A mesh is then placed to cover the hernia defect. The skin incisions are then closed with absorbable sutures.
Complications
Each approach has its own advantages and disadvantages, which will be discussed in detail at your consultation session. The greatest risk of undergoing hernia repair is that the hernia can come back (recurrence).
Fortunately, the recurrence rate is low with modern surgical techniques performed by experienced dedicated hernia surgeons.
Fortunately, the recurrence rate is low with modern surgical techniques performed by experienced dedicated hernia surgeons.
Postoperative care
The patient should expect to have some discomfort for one to two weeks. Therefore the patient will be discharged home with some oral pain relief. Patient is strongly encouraged to take regular pain relief in the first 7 days.
The only restriction in physical activity is not to do any heavy lifting for 3 weeks for a patient who has had an open hernia repair.
Patients who have had a laparoscopic hernia repair should not do any heavy lifting for 4 weeks. Please ask for more information.
Caution is also advised when participating in exercise.
The post-op care consultant will contact the patient 3–4 day after discharge from hospital.
The patient is typically reviewed 2–3 weeks after the operation.
Please also see: Hernia – overview
The only restriction in physical activity is not to do any heavy lifting for 3 weeks for a patient who has had an open hernia repair.
Patients who have had a laparoscopic hernia repair should not do any heavy lifting for 4 weeks. Please ask for more information.
Caution is also advised when participating in exercise.
The post-op care consultant will contact the patient 3–4 day after discharge from hospital.
The patient is typically reviewed 2–3 weeks after the operation.
Please also see: Hernia – overview
Clinical Associate Professor Hairul Ahmad MBBS FRACS
Upper Gastrointestinal, Advanced Laparoscopic and General Surgery
Perth, Western Australia
Perth, Western Australia
Practice Details
Suite 12, Waikiki Specialist Centre,
221 Willmott Drive, Waikiki WA 6169
Please call (08) 9592 2298 for an appointment.
Fax: (08) 6314 1524
or email us
Office hours
9am–4pm Monday to Friday
Affiliations



© 2022 Perth General Surgery.
All Rights Reserved. Content and images on this website are subject to copyright.